Get Complete Project Material File(s) Now! »
CHAPTER 2 LITERATURE REVIEW
INTRODUCTION
Literature review assists to summarize and understand the existing knowledge regarding the topic under study (Sadler, Burgin, McKinney & Ponjuan 2010:235). The literature review in this study serves to identify any gaps in the existing pool of knowledge on the topic under study. In this chapter the literature review covers the main concepts related to the research topic; specifically, diabetes mellitus, HIV, the relationship between HIV and DM, pregnancy care, effects of DM and HIV on pregnancy, and outcomes of pregnancy.The review was guided by the research questions. Google scholar, pubmed, UNISA electronic articles and books, national policy guides and reports on DM, HIV and maternal health were the source for the literature review. After thorough reading of these sources, summary notes were taken, similar themes were summarized and organized to fit to the reseach questions.
Non-communicable and communicable diseases in developing countries
The significant increase in non-communicable diseases death in the next decade is expected in Africa, where NCD is likely to become the leading cause of death by 2030 (Dalal, Beunza, Volmink, Adebamowo, Bajunirwe, Njelekela, Mozaffarian, Fawzi, Willett, Adami & Holmes 2011:885). However, less attention has been paid to the extent to which NCD contributed to morbidity and mortality. The focus in sub-Saharan Africa region has been on communicable diseases and maternal, perinatal and nutritional causes of morbidity and mortality (Boutayeb 2006:191). These are countries where the burden of communicable diseases is still high. The convergence of NCD and communicable diseases in low and middle income countries has the potential to overstretch the already strained health systems. With some developing countries now focusing on major health system reforms, a unique opportunity is available to address challenges by NCD and communicable disease with novel approaches. Therefore, integrating public health activities for communicable disease and NCD should extend beyond health care services to prevention (Remais, Zeng, Li, Tian & Engelgau 2013:221).
There are close relationships between communicable diseases and NCD in terms of causation, co-morbidity, and care. Oftentimes, both communicable diseases and NCD co-exist, and one can increase the risk or impact of the other (Norheim, Jha, Admasu, Godal, Hum, Kruk, Gómez-Dantés, Mathers, CD Pan, Sepúlveda and Suraweera. 2015:239). Diabetes, for example, can interact with and complicate a number of communicable diseases. HIV-infected patients with access to anti-retroviral treatments can now expect prolonged survival and ageing and hence accompanied by the emergence of diabetes and lipid disorders (Lo, Chen, Sheng, Hsieh, Sun, Liu, Wu, Wu, Hung & Chang, 2009:302).
Together, NCD and communicable disease can affect pregnancy outcomes. For instance, poor maternal nutrition before and during pregnancy together with smoking tobacco during pregnancy contribute to poor intrauterine growth, resulting in low birth weight which in turn predisposes to DM risk later in life. The problem is compounded by HIV/AIDS. Low birth weight and malnutrition are more frequent in HIV-infected children (DOS REIS et al 2015:111; Kim et al 2012:1). In this chapter DM, as an accelerating NCD; and HIV, as an impacting communicable disease will be discussed regarding their relationship and their impact on adverse pregnancy outcomes.
HUMAN IMMUNO-DEFICIENCY VIRUS
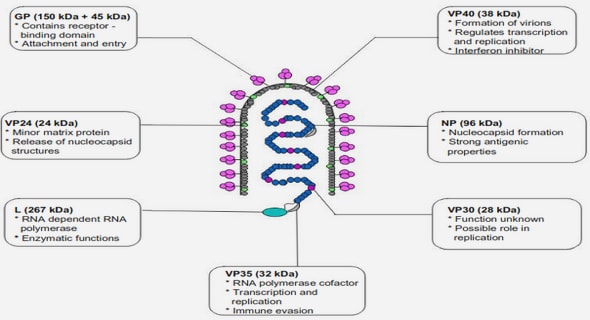
HIV belongs to the family of retroviruses that targets and weakens the immune system. The virus destroys immune cells with the CD4 (+) marker, often called T cells. Over time, HIV can destroy many of these cells to an extent that the body cannot fight off infectious diseases (WHO 2013a: xiv).The advanced stage of HIV infection is AIDS. AIDS is defined by the opportunistic infections or cancers that take advantage of a very weak immune system. It takes from 2 to 15 years to develop AIDS depending on the individual (Goldman & Ausiello 2008:393).
Transmission of HIV
HIV can be transmitted via the exchange of a variety of body fluids. The infectious fluids are blood, breast milk, semen and vaginal secretions. Having unprotected anal or vaginal sex; sharing contaminated needles, syringes and other injecting equipment and drug solutions when injecting drugs; receiving unsafe injections, blood transfusions, tissue transplantation, medical procedures that involve unsterile cutting or piercing; and experiencing accidental needle stick injuries can lead to HIV infection (Goldman & Ausiello 2008:395). The transmission of HIV from an HIV-positive mother to her child during pregnancy, labour, delivery or breastfeeding is called mother-to-child transmission (MTCT). Without interventions, the rate of HIV transmission from mother-to-child can be between 15-45% (Tsague, Tsiouris, Carter, Mugisha, Tene, Nyankesha, Koblavi-Deme, Mugwaneza, Kayirangwa, Sahabo & Abrams 2010:753).
Anti-retroviral medications
HIV can be suppressed by anti-retroviral therapy (ART) consisting of a combination of three or more anti-retroviral (ARV) drugs. ART does not cure HIV infection, but controls viral replication within a person’s body and allows an individual’s immune system to strengthen and regain the capacity to fight off infections (Goldman & Ausiello 2008:396).
HIV/AIDS and Chronic illnesses
The wide use and effectiveness of Highly Active Anti-retroviral Therapy (HAART) has allowed the HIV infected population to live a longer and healthier life. Thus, they are now exposed to the same amount of risk factors (increased age, obesity and lack of physical inactivity) for NCD such as DM and premature cardiovascular disease as the non-HIV infected population (Baker, Henry & Neaton 2009:176; Young et al 2009:9). The rate of NCD is becoming higher among HIV patients due to the high prevalence of traditional risk factors such as smoking, alcohol and substance abuse, adverse effects of certain ARV drugs such as Abacavir and some protease inhibitors and the direct effects of HIV itself (Alvarez, Salazar, Galindez, Rangel, Castañeda, Lopardo, Cuhna, Roldan, Sussman, Gutierrez & Cure-Bolt 2010:256).
In people living with HIV (PLHIV), there is chronic activation of the innate immune system with excessive production of inflammatory markers that in turn are associated with an increased risk of atherosclerosis and coronary artery inflammation. HIV-mediated breakdown of the integrity of the gut mucosa and chronic translocation of gut microbial products into the systemic circulation contribute to the chronic inflammatory state (Rajasuriar, Khoury, Kamarulzaman, French,Cameron & Lewin 2013:1199). These all pave a way to the development of chronic illnesses like DM among PLHIV.
DIABETIS MELLITUS
Diabetes is a serious, chronic disease that occurs either when the pancreas does not produce enough insulin; a hormone that regulates blood sugar or glucose, or when the body cannot effectively use the insulin it produces (Wiener, Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo & Brown 2012:1145).
Classification of Diabetes Mellitus
The WHO (2016:11) defines the following categories of diabetes mellitus:
- Type 1 diabetes (T1DM) which is characterized by deficient insulin production in the body. Type 1 diabetes patients require daily administration of insulin to regulate the amount of glucose in their blood. Symptoms include excessive urination and thirst, constant hunger, weight loss, vision changes and fatigue.
- Type 2 diabetes (T2DM) which is due to ineffective use of insulin. T2DM accounts for the vast majority of people with diabetes. It may go undiagnosed for several years, until complications have already arisen. For many years, T2DM was seen only in adults but it has begun to occur in children.
- Impaired glucose tolerance (IGT) and impaired fasting glycaemia (IFG) which are intermediate conditions that occur in the transition between normal blood glucose levels and diabetes (especially type 2), though the transition is not inevitable.
- Gestational diabetes mellitus (GDM) which occurs when a woman develops high blood sugar during pregnancy. It increases risk of infection and obstructed labour. If not properly treated, GDM can cause serious complications during pregnancy and childbirth. For instance, pre-eclampsia is three times more likely to occur in women with GDM (WHO 2016a:13).
Since GDM is associated with an increased risk for Type 2 diabetes for both the woman and child, it can also lead to serious health problems later in life. This can initiate a vicious cycle where the child will go on to have an increased risk of DM. This child also may pass this risk onto another generation (WHO 2016a:1).
Diabetes mellitus in Ethiopia
In Ethiopia, the International Diabetes Federation (IDF) 2015 report indicated an estimated DM prevalence of 3.4 % (IDF 2015:70). However, DM prevalence of as high as 8% has been reported in 2013 on HIV/AIDS patients taking HAART (Sachithanan, Loha & Gose 2013:1). DM claimed 23,145 deaths in Ethiopia in 2015 (IDF 2015:70).
A systemic review by Gebre (2013:249) in Ethiopia showed that Major DM related complications have increased; hypertension (12.1% to 34.1%), neuropathy (27.7% to 34.1%), and DM foot disease (1.7% to 4.6%). However, the review did not look into the complication of HIV on DM, or DM and HIV on pregnancy outcome. Hence, the researchers concluded mentioning that no study has been conducted confirming whether DM increases infectious disease occurrences or vice versa.
HIV AS A RISK FACTOR FOR DIABETES MELLITUS
The chronic and repeated inflammatory reaction by HIV correlates with an increased risk for diabetes. Some HAART medications have either direct or indirect adverse actions to a patient’s glucose metabolism, which makes them more likely to develop diabetes. Additional medications such as steroids given to treat some HIV-associated illness can cause altered glucose metabolism in healthy individuals (Tebas 2008:S86).
Another risk for insulin resistance in HIV-infected patients is Hepatitis C infection (White, Ratziu & El-Serag 2008:831). Due to the fact that both Hepatitis C and HIV are transmitted in the blood and risk factors for acquiring them are similar, some HIV-patients may be co-infected with hepatitis C (Operskalski & Kovacs 2011:12). Patients co-infected with both HCV and HIV had increased insulin resistance and higher diabetes rates versus HIV-infected patients without HCV infection after initiation of ART using a nucleoside reverse transcriptase inhibitor (NRTI) regimens with or without non-nucleoside reverse transcriptase inhibitor (NNRTI) (Butt, McGinnis, Rodriguez-Barradas, Crystal, Simberkoff, Goetz, Leaf & Justice 2009:1227).
The incidence of medication related diabetes increases as the duration of therapy increases. Protease inhibitors (PI) have a direct effect on glucose metabolism (hyperglycaemia) and then diabetes. Indinavir, ritonavir, and amprenavir are the PI’s commonly ascribed to diabetes (Ledergerber, Furrer, Rickenbach, Lehmann, Elzi, Hirschel, Cavassini, Bernasconi, Schmid, Egger & Weber 2007:111). Thus, the use of protease inhibitors has been associated with insulin resistance in pregnant and non-pregnant women. However, an association was not found between PI and Gestational diabetes (Jao, Wong, Van Dyke, Geffner, Nshom, Palmer, Muffih, Abrams, Sperling & LeRoith 2013: e141). The NRTI such as stavudine increases the risk for developing diabetes indirectly as well (Ledergerber et al 2007:111; Young et al 2009:9).
Incidence and risk factors of DM among HIV patients
According to the population survey in America, DM prevalence among HIV-infected adults was 10.3% and this was 3.8% (95% confidence interval (95% CI): 1.8% to 5.8%) higher in HIV-infected adults compared with general population adults. The survey shows that DM among HIV-infected persons may develop at earlier ages in the absence of obesity. Among HIV-infected adults with diagnosed DM, 3.9% had DM type 1 and 52.3% had DM type 2 and 43.9% had unspecified DM. Factors independently associated with DM among HIV-infected adults include increasing age, obesity, increasing time since HIV diagnosis, and geometric mean of CD4 (+) count. ART prescription in the past year is not associated with prevalent DM in the survey (Hernandez-Romieu, Garg, Rosenberg, Thompson-Paul and Skarbinski 2017: e000304).
CHAPTER 1 ORIENTATION TO THE STUDY
1.1 INTRODUCTION
1.2 BACKGROUND TO THE RESEARCH PROBLEM
1.3 STATEMENT OF THE RESEARCH PROBLEM
1.4 PURPOSE OF THE STUDY
1.5 RESEARCH QUESTIONS
1.6 SIGNIFICANCE AND CONTRIBUTION OF THE STUDY
1.7 DEFINITIONS OF KEY CONCEPTS
1.8 ASSUMPTIONS OF THE STUDY
1. 9 THOERETICAL FRAMEWORK
1.10 RESEARCH PARADIGMS
1.11 THE RESEARCH DESIGN
1.12 RESEARCH METHODS
1.13 LAYOUT OF THE STUDY
1.14 CONCLUSION
CHAPTER 2 LITERATURE REVIEW
2.1 INTRODUCTION
2.2 HUMAN IMMUNO-DEFICIENCY VIRUS
2.3. DIABETIS MELLITUS
2.4 HIV AS A RISK FACTOR FOR DIABETES MELLITUS
2.5 PREGNANCY AND MATERNAL HEALTH
2.6 ADVERSE PREGNANCY OUTCOMES
2.7 CONCLUSION
CHAPTER 3 RESEARCH DESIGN AND METHOD
3.1 INTRODUCTION
3.2 RESEARCH DESIGN
3.3 A MIXED METHOD APPROACH
3.4 QUALITATIVE RESEARCH APPROACH.
3.6 RESEARCH METHOD.
3.7 ETHICAL CONSIDERATION
3.8 CONCLUSION
CHAPTER 4 PRESENTATION, DESCRIPTION AND TRIANGULATION OF THE FINDINGS
4.1 INTRODUCTION
4.2 PHASE I
4.3 PHASE II
4.4 COMBINED FIDINGS OF FGDs, IDIs AND OBSERVATIONS
4.5 LEVEL OF DM, HIV AND PREGNANCY CARE INTEGRATION
4.6 PRESENTATION AND DESCRIPTION OF FINDINGS IN PHASE II
4.7 DESCRIPTION AND TRIANGULATION OF PHASE I AND PHASE II FINDINGS
CHAPTER 5 DEVELOPMENT OF AN INTEGRATED SERVICE DELIVERY MODEL FOR HIV, DM AND PREGNANCY CARES
5.1 BACKGROUND TO THE MODEL DEVELOPMENT.
5.2 PURPOSE OF THE MODEL DEVELOPMENT
5.3 COMPONENTS OF THE MODEL
5.4 BUILDING THE MODEL
5.5.1 Experts participated in the evaluation of the model
5.6 THE COMPARISON OF THE INTEGRATED THEORETICAL FRAMEWORK AND THE TRIPARTITE SERVICE DELIVERY MODEL FOR HIV, DM AND PREGNANCY CARE
5.7 CONCLUSION
CHAPTER 6 CONCLUSIONS, LIMITATIONS AND RECOMMENDATIONS
6.1 INTRODUCTION
6.2 RESEARCH DESIGN AND METHOD
6.3 SUMMARY AND INTERPRETATION OF THE RESEARCH FINDINGS
6.4 CONTRIBUTION OF THE STUDY
6.5 LIMITATIONS
6.7 CONCLUDING REMARKS
6.8 COMMUNICATING THE FINDINGS
LIST OF REFERENCES
GET THE COMPLETE PROJECT