Get Complete Project Material File(s) Now! »
Induction of ICD sensitize cancers to immune checkpoint blockade
Immunotherapy, particularly immune checkpoint blockade (ICB), is now largely applied to treat various cancers. But due to the immunosuppressive nature of tumour microenvironment, the objective response rates (ORRs) of standard ICB treatment in solid tumours are relatively low (Lim et al., 2016; Rosenberg et al., 2016; Topalian et al., 2012). ICD induction in tumour sites enables to recruit antigen presenting cells and CD8 T cells to the tumour bed, thus convert immunologically ‘cold’ tumours into ‘hot’ lesions. Given that ICB’s therapeutic function dedicated to the presence of CD8 T cells, pre-treatment with ICD inducers sensitize tumours to ICB in several studies (Liu et al., 2019; Pfirschke et al., 2016; Yamazaki et al., 2020).
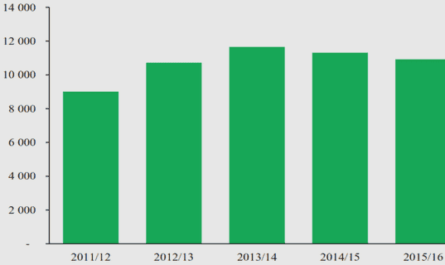
In a cohort of NSCLC patients, chemoradiotherapy plus programmed death-ligand 1 (PD-L1) blockade dramatically prolonged the overall survival of combination treatment group against placebo group (Antonia et al., 2018). In another study involves metastatic triple-negative breast cancer patients, doxorubicin treatment upregulates the expression of key genes which related to programmed cell death protein 1 (PD-1)/PD-L1 and T cell cytotoxicity pathways, thus evaluated the objective response rate to PD-1 blockade (Voorwerk et al., 2019). In addition, bunch of clinical trials that involves the combination of immunogenic chemotherapy and ICBs are still ongoing (Galluzzi et al., 2020a)(Figure 10).
Altogether, both preclinical and clinical studies reveal that ICD-inducing chemotherapy may bring benefits to cancer patients in some immunotherapy included settings. But the optimal therapeutic combination regiments remain to be critically evaluated.
Figure 10. Overview of ongoing clinical trials involving one or more immunogenic cell death inducers in combination with immune checkpoint inhibitors in patients with cancer. As of 1 March, 2020, ClinicalTrials.gov listed 55 ongoing (defined as those that are not completed, withdrawn, suspended, terminated or have unknown status) clinical trials in which patients are receiving chemotherapy plus agents with known immunogenic cell death (ICD)-inducing potential in combination with one or more FDA-approved immune checkpoint inhibitors in patients with cancer that were initiated after 1 January, 2019. CTLA4, cytotoxic T lymphocyte-associated protein (Galluzzi et al., 2020a).
Transcription inhibitor Lurbinectedin
Lurbinectedin (PM01183) is a novel synthetic marine-derived anticancer agent developed by PharmaMar Company. It was recently approved by Federal Drug Administration (FDA) for the salvage treatment of small-cell lung cancer (SCLC). As an alkaloid, lurbinectedin could binds to the DNA minor groove, induces double-strand DNA breaks, selectively blocks RNA polymerase II activity and promotes its degradation, disrupts mitosis and eventually induces cell death (Leal et al., 2010; Santamaria Nunez et al., 2016; Vidal et al., 2012). As an analogue of trabectedin, the structure of lurbinectedin is similar to trabectedin except the modification in C subunit (Leal et al., 2010). Thus, lurbinectedin gains different pharmacokinetic and pharmacodynamics properties from trabectedin (Bueren-Calabuig et al., 2011; Leal et al., 2010; Soares et al., 2011).
It’s reported that lurbinectedin has potent antiproliferative activity in numerous cancer cell lines in vitro, including cisplatin-sensitive and resistant cells (Leal et al., 2010; Santamaria Nunez et al., 2016; Soares et al., 2011). Single lurbinectedin treatment exhibits antitumor/antimetastatic activity in MNMCA1, M5076 murine reticulosarcoma, HOC8 and MNBPTX human ovarian carcinoma xenograft in vivo (Romano et al., 2013). In preclinical uterine cervical cancer models, lurbinectedin inhibits tumour growth by eliminating both cancer stem cell and non-cancer stem cell (Yokoi et al., 2019). Lurbinectedin inactivates oncoprotein EWS-FLI1 and synergized with irinotecan to retard Ewing sarcoma xenograft growth (Harlow et al., 2016). Also, lurbinectedin therapy overcomes cisplatin resistance in in epithelial ovarian cancer (Vidal et al., 2012). In particular, lurbinectedin depletes tumour-associated macrophages and modulates inflammatory microenvironment in both mouse fibrosarcoma tumour model and patient-derived (AVATAR) PDA xenografts (Belgiovine et al., 2017; Cespedes et al., 2016; Farago et al., 2019)(Figure 11).
Figure11. Chemical structure and schematized actions of lurbinectedin. (A) Chemical structure of lurbinectedin. (B) Schematic representation of lurbinectedin mechanism of action for binding DNA, inhibiting active transcription and inducing DNA breaks. (C) Schematic representation of lurbinectedin interactions with the tumor microenvironment. Lurb: Lurbinectedin (Farago et al., 2019).
The approval of lurbinectedin for second line SCLC treatment was based on several clinical trials. In a Phase I study enrolled 27 relapsed SCLC patients, the combination regiment of lurbinectedin and doxorubicin showed remarkable anticancer activity. As second-line treatment, 11 out of 12 patients with platinum-sensitive disease and 3 out of 9 patients with platinum-resistant disease were responded to the combination treatment (Calvo et al., 2017). In a single-arm, open-label phase II basket trial, 105 patients with relapsed SCLC were treated with lurbinectedin alone. The median overall survival (OS) was 9.3 months, 11.9 months, 5.0 months in the whole cohort, patients with chemotherapy sensitive or resistant disease respectively. Among all patients the overall response rate (ORR) was 35.2%, whereas 45.0% in chemotherapy sensitive subgroup and 22.2% in chemotherapy resistant subgroup. Further, lurbinectedin was of good safety, no patient dead due to treatment related advise effects (Trigo et al., 2020). It’s notable that the combination therapy of lurbinectedin and atezolizumab (anti-PD-L1 antibody) in patients with progressed SCLC is under evaluation (ClinicalTrials.gov, NCT04253145). Apart from SCLC, lurbinectedin is in therapeutic trials for multiple cancer types, including breast cancer, ovarian cancer, sarcoma, acute leukaemia and different advanced solid tumours (Markham, 2020)(Table 3).
Oncolytic peptide LTX-401
Antimicrobial peptides (AMPs) are a series of short cationic amphipathic peptides that protect hosts from various microorganisms (Fjell et al., 2011; Hancock and Sahl, 2006). More than 2000 kinds of natural AMPs were discovered currently, but no conserved motif or sequence has been identified yet (Wang et al., 2016). Apart from anti-microorganism activity, some AMPs exert anticancer property by directly lysing cancer cells (Al-Benna et al., 2011; Gaspar et al., 2013). Bovine lactoferricin (LfcinB) is the best studied natural AMP which is derived from milk protein. It’s reported that LfcinB could induce cancer cell necrosis and apoptosis by destabilise membranes (Eliassen et al., 2006; Eliassen et al., 2002; Mader et al., 2005; Yoo et al., 1997). Based on the structure of LfcinB, a large number of oncolytic peptides were designed and synthetized to treat cancer. One of these oncolytic peptides is LTX-401, an amphiphatic β (2,2)-amino acid derivate that is able to lysis different type of cells (Eike et al., 2016) (Figure 12).
Previous data demonstrated that LTX-401 preferentially enriches in Golgi apparatus and destroys its structure, subsequently inducing cell death. The presence of brefeldin A (BFA) reduces the cytotoxicity of LTX-401 not only due to the prophylactic dissociation of Golgi, but also through decreasing mitochondrial permeabilization. BAX/BAK deficient or mitochondrial depleted cells show partial resistance to LTX-401 mediated killing, while pan-caspase inhibitor Z-VAD-fmk doesn’t exhibit any protective effect (Zhou et al., 2016b). In addition, LTX-401 treatment impairs lysosomal integrity and induces the release of reactive oxygen species (ROS).
Massive DAMPs are released following LTX-401 treatment, including ATP, Type I IFN, HMGB1, cytochrome c and CALR exposure. Intra-tumour injection of LTX-401 causes focal necrosis and T lymphocytes infiltration (Eike et al., 2016; Mauseth et al., 2019; Zhou et al., 2016b).
The antitumor capacity of LTX-401 were verified in several cancer models. Local administration of LTX-401 in 3 consecutive days cured more than 80% of B16F1 melanoma (Eike et al., 2016). In subcutaneous JM1 tumour model, 7 out of 10 tumours were completed regressed post LTX-401 treatment. All cured animals were resistant to both subcutaneous and intrahepatic rechallenge of the same tumour cell. More convincing date was obtained from rat orthotopic JM1 liver cancer model, a preclinical model of human hepatocellular carcinoma (HCC). 5 out of 9 mice were cured from orthotopic JM1 liver tumour, by intrahepatic injection of LTX-401 on day 6 and day 8 post tumour incubation. Again, cured mice generated long-term antitumor immunity (Mauseth et al., 2019).
AIMS OF THE THESIS
Cancer cells undergo immunogenic cell death effectively provoke anticancer immune response in immunocompetent host. Therefore, ICD inducers could somehow convert dying tumour cells to therapeutic ‘vaccines’, attracting leukocytes to tumour beds and thus switching from the immunosuppressive tumour microenvironment to a proinflammatory context. In addition, both preclinical study and clinical trials support the hypothesis that pre-treatment with a panel of ICD inducers sensitize tumours to immune checkpoint blockade.
Based on this rationale, it’s of great value to evaluate the capacity of drugs/compounds in inducing ICD and potential benefits in combination with ICBs.
Lurbinectedin is a RNA polymerase II inhibitor which was newly approved by FDA for cancer treatment. The majority of previous studies investigated its anticancer ability in immunodeficient host, thus the immunogenicity of lurbinectedin induced cell death is still unknown.
As an oncolytic peptide, LTX-401 is designed for local administration. Past research shows that LTX-401 could selectively concentrate in and destroy Golgi apparatus, inducing all the hallmarks of ICD in vitro. But the capacity of LTX-401 to stimulate anticancer immune responses remains to be elucidated.
The specific aims of this thesis are:
To evaluate the capacity of lurbinectedin in stimulating the hallmarks of ICD.
To investigate the anticancer immune responses of lurbinectedin and LTX-401 in different experimental cancer models.
To explore the combination therapeutic regiments in cancer treatment.
RESULTS
Lurbinectedin synergizes with immune checkpoint blockade to generate anticancer immunity Accumulating results indicate that chemotherapeutic drugs which efficiently inhibit transcription and promote eIF2α phosphorylation are potent ICD inducers, indicating the potential of lurbinectedin in inducing ICD. Both preclinical data and clinical trials demonstrate that pre-treatment with certain ICD inducers sensitizes to immune checkpoint blockade, it’s worthwhile to investigate the role of lurbinectedin in the era of immunotherapy.
To evaluate the immunogenicity of lurbinectedin, different parameters of ICD hallmarks were measured by robotized epifluorescence microscopy followed by automated image analysis. Lurbinectedin triggered CALR exposure, ATP release, HMGB1 exodus, Type I IFN release and cell death in a dose- and time-dependent manner in 4 human or mouse cancer cell lines. Also, lurbinectedin activated two ICD pathways named split ER stress and transcription inhibition, featured by elevated eIF2α phosphorylation level and decreased co-localization of nucleolin and fibrillarin. Thus, Lurbinectedin induced all traits of ICD in vitro. To further confirm its immunogenicity in vivo, we employed the vaccination experiment in immunocompetent mice. Lurbinectedin-treated cells significantly reduced tumour growth and led to increased overall survival.
Next, we investigated the therapeutic efficacy of lurbinectedin in immunocompetent and immunodeficient mice. Lurbinectedin significantly retarded MCA205 tumour growth and extended survival span in immunocompetent host but failed to do so in immunodeficient counterpart. Implying that the anticancer efficiency of lurbinectedin in MCA205 cancer depends on immune system.
Moreover, lurbinectedin, αCTLA-4 and αPD-1 triple combination regiment dramatically inhibited tumour progression and induced complete regression in 3 out of 8 animals. Cured mice exhibited systemic antitumor immunity to the same type of cancer cell. In particular, T lymphocyte depletion abolished the effect of lurbinectedin with αCTLA-4/αPD-1 dual checkpoint blockade.
Finally, we tested the therapeutic effect of lurbinectedin in MPA/DMBA-induced spontaneous breast cancer model. Both lurbinectedin alone and in combination with double ICBs significantly reduced tumour growth and increased overall survival.
Table of contents :
INTRODUCTION
Cancer and anticancer immunity
Cancer epidemiology
Cancer immunology
Immunogenic cell death in cancer therapy
Major DAMPs of ICD
Methods to detect ICD
ICD inducers
Induction of ICD sensitize cancers to immune checkpoint blockade
Transcription inhibitor Lurbinectedin
Oncolytic peptide LTX-401
AIMS OF THE THESIS
RESULTS
Lurbinectedin synergizes with immune checkpoint blockade to generate
anticancer immunity
Tumor lysis with LTX-401 creates anticancer immunity
CONCLUDING REMARKS
ACKNOWLEDGEMENT
REFERENCES
ANNEX 1: SCIENTIFIC PUBLICATIONS
ANNEX 2: PAPERS NOT INCLUDED IN THIS THESIS (INSERTED IN PDF)