Get Complete Project Material File(s) Now! »
Background
A worldwide drop in mortality rates and rise in life expectancy have increased society‟s attention on reducing disability and handicap, including deafness and hearing impairment (Goulios & Patuzzi, 2008). Hearing loss ranks as the number one cause of disability globally with 10% of the global population presenting with a mild or greater hearing loss (World Health Organization [WHO], 2006, 2010). Adult-onset hearing loss is ranked thirteenth amongst the leading causes of the global burden of disease, and ninth in terms of years of healthy life lost as a result of disability (Lopez, Mathers, Ezzati, Jamison, & Murray, 2006; Mathers & Loncar, 2006). More than half the global burden of hearing impairment may be caused by preventable ear disease, specifically chronic suppurative otitis media (CSOM; Acuin, 2004). If untreated, where secondary complications are possible, ear disease may lead to sensorineural hearing loss.
Ear disease
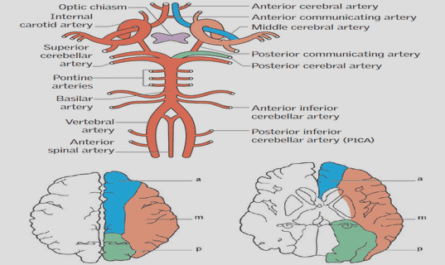
The WHO classifies ear disease into three categories: diseases of the external ear; diseases of the middle ear and mastoid; and diseases of the inner ear (Centre for Disease Control and Prevention, 2013). Diseases of the external ear include disease of both the pinna and the external auditory meatus. The external auditory meatus may present with cerumen impaction, a foreign object, otitis externa or exostosis (Silverberg & Lucchesi, 2011). Middle ear disease includes Eustachian tube disorders, otitis media, cholesteatoma, otosclerosis and other ossicular disorders (Swarts et al., 2013; Yoon, Patricia, Kelley, & Friedman, 2012). Tympanic membrane pathologies fall under middle ear disease, and may include conditions such as myringitis, myringosclerosis, retraction pockets and perforations (Jung et al., 2013; Yoon, Patricia et al., 2012). Mastoiditis is a secondary complication of otitis media. Inner ear diseases include disorders of both the cochlear and the vestibular system (Verhoeff, van der Veen, Rovers, Sanders, & Schilder, 2006).
Models of service delivery
Three distinct telehealth practice models are recognized namely store-and-forward (asynchronous), clinician interactive (synchronous), and self-monitoring/testing (Agency for Healthcare Research and Quality, 2001). A combination of both synchronous and asynchronous approaches may also be useful in some settings (Krumm, 2007).
Video-otoscopy within telehealth clinics
Studies comparing video-otoscopy with conventional face-to-face otoscopy examination concluded that images are equivalent in quality to standard face-to-face otoscopy, with 75% to 82% judged to be of adequate quality or better (Lundberg, Westman, Hellström, & Sandström, 2008; Pedersen, Hartviksen, & Haga, 1994; Smith, Perry, Agnew, & Wootton, 2006). Importantly, for the purpose of validation of use of video-otoscopy within a teleaudiology program, studies have demonstrated average to good diagnostic concordance between otoscopy and video-otoscopy images (Burgess et al., 1999; Eikelboom et al., 2005; Kokesh et al., 2008; Patricoski et al., 2003).
ACKNOWLEDGMENTS
ABSTRACT
1 INTRODUCTION
1.1 Background
1.2 Ear disease
1.3 Otitis media
1.4 Telehealth
1.5 Models of service delivery
1.6 Video-otoscopy within telehealth clinics
1.7 Rationale
2. METHOD
2.1 Research objectives
2.2 Research design and methods
2.3 Ethical considerations
3. STUDY I: Asynchronous video-otoscopy by a telehealth facilitator
3.1 Abstract
3.2 Introduction
3.3 Materials and methods
3.3.1 Population
3.3.2 Data collection
3.3.3 Data analyses
3.4 Results
3.5 Discussion
3.6 Conclusion
3.7 Acknowledgements
3.8 References
4. STUDY II: Video-otoscopy recordings for diagnosis of childhood ear disease using telehealth at primary health care level
4.1 Abstract
4.2 Introduction
4.3 Materials and methods
4.3.1 Otomicroscopic examination
4.3.2 Video-otoscopy recordings
4.3.3 Equipment
4.3.4 Asynchronous assessment
4.3.5 Analyses
4.4 Results
4.5 Discussion
4.5.1 Quality of video-otoscopy recordings
4.5.2 Diagnostic accuracy using video-otoscopy recordings
4.6 Conclusion
4.7 Acknowledgements
4.8 References
5. STUDY III: Paediatric otitis media at a primary health care clinic in South Africa
5.1 Abstract
5.2 Introduction
5.3 Method
5.3.1 Population
5.3.2 Data collection
5.3.3 Data analysis
5.4 Results
5.5 Discussion
5.6 Conclusion
5.7 References
6. SUMMARY AND CONCLUSIONS
6.1 Summary of study findings
6.2 Clinical implications
6.3 A telehealth model for primary health care diagnosis of ear disease
6.4 Study strengths and limitations
6.4.1 Study strengths
6.4.2 Study limitations
6.5 Recommendations for further research
6.6 Conclusion
7. REFERENCES
8. APPENDICES
GET THE COMPLETE PROJECT
TELEHEALTH FOR PRIMARY HEALTH CARE EAR DISORDERS: A STUDY IN VIDEO-OTOSCOPY