Get Complete Project Material File(s) Now! »
Data Analyses
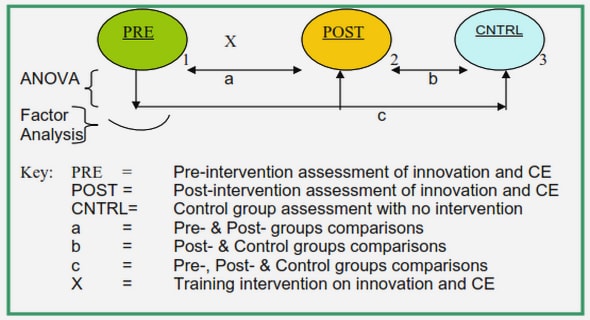
The data analyses included several independent analysis of variance (ANOVA) procedures using data from all focus groups (NO, FL, FR), which were followed by several refined analyses of variance for each group (ANOVAs), explained below. Post hoc comparisons were performed on all means with Tukey’s Honestly Significant Difference procedure (HSD; a = .05). Significant differences are indicated by dissimilar letters on the bars within the ensuing figures / graphs.
Self Report Scales
A t-test was conducted to assess differences between men and women on the Cook-Medley Hostility Inventory, used as a descriptive measure in this study to further explore subject variables related to cardiovascular reactivity and disease. T-tests were also conducted on CPD scores, MCSDS scores, and age of participant for each sex to discover if any significant differences existed between men and women on any of these descriptive measures.
Physiological Measures
Independent analyses of variance (ANOVA) were performed on the physiological variables (HR, SBP, and DBP) to measure cardiovascular reactivity to the cold pressor. There were three statistical designs analyzing: A) overall group effects (using all focus groups), B) focus effects on cardiovascular reactivity (using focus left and focus right groups), and C) sex differences in cardiovascular reactivity among the no focus (control) groups.
Statistical analysis design A was: Sex (2 levels) x Focus (3 levels) x Condition (4 levels). Thus, data were analyzed with a three-factor mixed design, analysis of variance (ANOVA), with fixed factors of Sex (men and women) and Focus (NO, FL, FR), and a repeated measure of Condition (baseline, post dichotic 1, post cold pressor, and post dichotic 2; see Figure 1). In addition, more refined ANOVAs were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD and significant differences are indicated by dissimilar letters on graphs.
Statistical analysis design B was: Sex (2 levels) x Focus (2 levels) x Condition (4 levels) . Thus, data were analyzed with a three-factor mixed design, analysis of variance (ANOVA), with fixed factors of Sex (men and women) and Focus (FL and FR), and a repeated measure of Condition (baseline, post dichotic 1, post cold pressor, and post dichotic 2). In addition, refined ANOVAS were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Significant differences are indicated by dissimilar letters on graphs.
Statistical analysis design C used only NO focus participants and was: Sex (2 levels) x Condition (4 levels). Thus, data were analyzed with a two-factor mixed design, analysis of variance (ANOVA), with a fixed factor of Sex (men and women), and a repeated measure of Condition (baseline, post dichotic 1, post cold pressor, and post dichotic 2). In addition, refined ANOVAS were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Again, significant differences are indicated by dissimilar letters on graphs.
Dichotic Listening Scores: POC
From the dichotic listening scores a percentage of correct responses (POC) index was calculated to assess the percent of correctly identified speech sounds by each participant. This was computed according to the following formula: POC = (pR – pL) / (pR + pL)
where: pR = proportion of correctly identified right-ear stimuli pL = proportion of correctly identified left-ear stimuli POC scores fall within a range of +1 (right ear advantage, a perfect score) to -1 (left ear advantage, a perfect score). An independent analysis of variance (ANOVA) was performed on the dependent variable obtained through the dichotic listening task- percent of correct responses (POC) score. Again, there were three statistical designs analyzing:
overall group effects (using all focus groups), B) focus effects on POC scores (using focus left and focus right groups), and C) sex differences in POC scores among the no focus (control) groups.
Statistical analysis design A was: Sex (2 levels) x Focus (3 levels) x Trial (2 levels). Thus, data were analyzed with a three-factor mixed design analysis of variance (ANOVA), with fixed factors of Sex (men and women) and Focus (NO, FL, FR), and a repeated measure of Trial (dichotic 1 pre-stressor vs. dichotic 2 post-stressor). In addition, more refined ANOVAS were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Significant differences are indicated by dissimilar letters on graphs.
Statistical analysis design B was: Sex (2 levels) x Focus (2 levels) x Trial (2 levels). Thus, data were analyzed with a three-factor mixed design analysis of variance (ANOVA), with fixed factors of Sex (men and women) and Focus (FL and FR), and a repeated measure of Trial (dichotic 1 pre-stressor vs. dichotic 2 post-stressor). In addition, more refined ANOVAS were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Significant differences are indicated by dissimilar letters on graphs.
Statistical analysis design C used only NO focus participants and was: Sex (2 levels) x Trial (2 levels). Thus, data were analyzed with a two-factor mixed design analysis of variance (ANOVA), with a fixed factor of Sex (men and women), and a repeated measure of Trial (dichotic 1 pre-stressor vs. dichotic 2 post-stressor). In addition, more refined ANOVAS were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Again, significant differences are indicated by dissimilar letters on graphs.
Dichotic Listening Scores: Dichotic Left and Dichotic Right
Independent analyses of variance (ANOVAs) were performed on dichotic listening task variables (number of correctly identified stimuli presented to the left ear and to the right ear). There were three statistical designs analyzing: A) overall group effects (using all focus groups); B) focus effects on dichotic listening scores (using focus left and focus right groups); and C) sex differences in dichotic listening scores reactivity among the no focus (control) groups.
Statistical analysis design A was: Sex (2 levels) x Focus (3 levels) x Trial (2 levels). Thus, data were analyzed with a three-factor mixed design, analysis of variance (ANOVA) with fixed factors of Sex (men and women) and Focus (NO, FL, FR), and a repeated measure of Trial (dichotic 1 pre-stressor vs. dichotic 2 post-stressor). In addition, more refined ANOVAs were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Significant differences are indicated by dissimilar letters on graphs.
Statistical analysis design B was: Sex (2 levels) x Focus (2 levels) x Trial (2 levels). Thus, data were analyzed with a three-factor mixed design, analysis of variance (ANOVA) with fixed factors of Sex (men and women) and Focus (FL and FR), and a repeated measure of Trial (dichotic 1 pre-stressor vs. dichotic 2 post-stressor). In addition, more refined ANOVAs were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Significant differences are indicated by dissimilar letters on graphs.
Statistical analysis design C used only NO focus participants and was: Sex (2 levels) x Trial (2 levels). Thus, data were analyzed with a two-factor mixed design, analysis of variance (ANOVA) with a fixed factor of Sex (men and women) and a repeated measure of Trial (dichotic 1 pre-stressor vs. dichotic 2 post-stressor). In addition, more refined ANOVAs were performed for each sex. Post hoc comparisons were performed with Tukey’s HSD. Again, significant differences are indicated by dissimilar letters on graphs.
Results
Descriptive Measures
In order to assess possible sex differences on the descriptive measures, t-tests were performed. There was no significant difference between the mean age of men (M = 19.47 years, SD = 1.29) and women (M = 19.45 years, SD = 1.20), t(118) = 0.10, p < .92.
There was no significant difference between men’s and women’s mean score on the Coren, Porac, and Duncan Laterality Questionnaire, (M = 10.3, SD = 2.0) and (M =11.0, SD = 2.3), respectively, t(118) = -1.73, p < .09. There was a nonsignificant trend for women to be more strongly right handed than men.
On the Marlowe-Crowne Social Desirability Scale men (M = 14.7, SD = 4.7), and women (M = 16.3, SD = 5.7) were not significantly different, t(118) = -1.66, p < .10.
However, scores obtained from the Cook-Medley Hostility Inventory (CMHO) indicate that men, as a group, were more hostile than women. Men scored significantly higher (M = 20.4, SD = 7.2) than women (M = 17.3, SD = 6.9), T(118) = 2.38, p < .02. This scale was included as a descriptive measure in this study to further explore subject variables related to cardiovascular reactivity and disease. It has been used extensively for this purpose (Williams & Anderson, 1987). Inclusion of this measure was useful in the preparation for a follow-up study that will investigate sex differences in the effects of hostility on cardiovascular reactivity.
Cardiovascular Reactivity
In order to assess cardiovascular reactivity, independent analyses of variance (ANOVAs) were performed on the following dependent variables of cardiovascular reactivity: systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR). Recall that data were analyzed in the following three design sequences: A) overall group effects (using all focus groups); B) focus effects on cardiovascular reactivity (using focus left and focus right groups only); and C) cardiovascular reactivity in the no focus (control) groups. Further, in each design, refined ANOVAs were performed for each sex. The following results are from statistical analysis design sequence A.
Group means and standard deviations of SBP, DBP, and HR measures are presented in Tables 1, 2 and 3, respectively. Independent ANOVA results of these cardiovascular measures are presented in Table 4.
A main effect of sex was found for both systolic blood pressure and diastolic blood pressure. Overall, men evidenced significantly higher SBP than women (M = 126.32 vs. 113.56, F (1,114) = 46.04, p < 0.0001). However, women evidenced significantly higher DBP than men (M = 75.91 vs. 68.26, F (1,114) = 27.74, p < 0.0001). A main effect of sex was not found for HR.
A main effect of focus was found only for DBP, F (2,114) = 3.73, p < 0.0271, where the Focus Right (FR) groups evidenced the lowest DBP (see Figure 2). Nevertheless, the Focus Left groups were significantly different from the No Focus groups, whereas, the Focus Right groups did not differ significantly from the No Focus groups in DBP.
A main effect of Condition was found for SBP (F (3,342) = 75.85, p < 0.0001), DBP (F (3,342) = 14.54, p < 0.0001), and HR (F (3,342) = 6.76, p < 0.0002), with significant changes occurring between experimental conditions. Therefore, all cardiovascular measurements during various conditions were significantly different from one another. These significant changes are detailed below.
Overall, across all focus groups, systolic blood pressure (SBP) decreased significantly between Condition 1 (baseline) and Condition 2 (post dichotic 1). A significant increase in SBP occurred across groups at Condition 3 (post cold pressor), followed by another significant decrease in SBP at Condition 4 (post dichotic 2), indicating systolic recovery from the cold pressor (see Figure 3)
Diastolic blood pressure (DBP) did not show a significant change between Condition 1 (baseline) and Condition 2 (post dichotic 1). A significant increase in DBP did occur across groups at Condition 3 (post cold pressor), followed by a significant decrease in DBP at Condition 4 (post dichotic 2), indicating diastolic recovery from the cold pressor (see Figure 4).
Heart rate (HR) did not change significantly between Condition 1 (baseline) and Condition 2 (post dichotic 1), in the three focus groups analyzed together. However, a significant decrease in HR occurred across groups at Condition 3 (post cold pressor), followed by a significant increase at Condition 4 (post dichotic 2; see Figure 5). This might suggest a healthy cardiovascular reactivity response across participants. Heart rate and blood pressure are inversely related through the baroreceptor reflex (Rushmer, 1976). That is to say, as blood pressure increased as a function of the cold pressor (SBP and DBP), heart rate decreased, compensating for some of the extra pressure effects in the vasculature.
Refined independent analyses of variance (ANOVAs) were then performed for each sex and are presented in Table 5. For men, a focus main effect on SBP was found, F (2,57) = 4.39, p < 0.0169, where the focus right participants experienced significantly lower SBP than the focus left participants (see Figure 6). Thus, the men showed a cardiovascular response which suggests more lateralized SBP control. This effect also lends support to theories on greater functional cerebral laterality in men, as focusing on speech sounds heard in the right or the left ear (a selective attentional task) produced different effects on systolic blood pressure. These focus effects were different for each sex, as women did not evidence a focus main effect on SBP.
The first dichotic listening test occurred between Conditions 1 and 2 (baseline vs. post dichotic 1), which corresponded with a significant decrease in men’s systolic blood pressure at Condition 2 (see Figure 7). However, women did not evidence a similar decrease at Condition 2 as a function of the dichotic listening test (see Figure 8). This difference in main effects for each sex supports the idea that language and/or parasympathetic cardiovascular regulation is more lateralized to the left hemisphere in men, since the left hemisphere was likely activated by the language task and then systolic blood pressure evidenced a drop in men between Conditions 1 and 2. Overall, for men and for women, a main effect of Condition was found for SBP (for men, F (3,171) = 52.25, p < 0.0001; and for women, F (3,171) = 26.44, p < 0.0001).
The main effect of Condition found for DBP was also significant for men and for women, F (3,171) = 5.69, p < 0.0010, and F (3,171) = 9.12, p < 0.0001, respectively.
For women, a main effect of Condition on HR was found, F (3,171) = 6.46, p < 0.0004, where HR decreased significantly following the cold-pressor (at Condition 3). However, men did not evidence a main effect of Condition on HR. As stated previously, a drop in HR as SBP increases is a healthy response pattern. Therefore, it is interesting that men did not evidence this (arguably) healthy cardiovascular response pattern.
Literature Review
Rationale
Experiment
Variables
Hypotheses
Method
Participant Selection
Measures
Apparatus
Cold Pressor
Dichotic Listening
Hearing
Physiological.
Procedure
Analyses
Results
Discussion
References
GET THE COMPLETE PROJECT
CARDIOVASCULAR REACTIVITY TO SPEECH PROCESSING AND COLD PRESSOR STRESS: EVIDENCE FOR SEX DIFFERENCES IN DYNAMIC FUNCTIONAL CEREBRAL LATERALITY