Get Complete Project Material File(s) Now! »
Background
In order to explore the usefulness of SPC for quality improvement work in psychiatry, the following paragraphs describe what QI is and explore its scientific basis through taking a closer look at Deming´s ‘profound knowledge’ (1994) and its four elements needed in QI: ‘appreciation of a system’, ‘understanding variation’, ‘theory of knowledge’ and ‘psychology’. Further follows elaboration on how to make use of variation by using SPC and control charts before the use of SPC in psychiatry is explored, looking at published articles.
On Quality Improvement (QI) and the Science of Quality Improvement
QI in health care could be defined as “the combined and unceasing efforts of everyone—healthcare professionals, patients and their families, researchers, payers, planners and educators— to make the changes that will lead to better patient outcomes (health), better system performance (care) and better professional development (learning)” (Batalden & Davidoff, 2007, p.2). Two bases of knowledge are needed, according to Batalden and Stoltz (1993), the professional knowledge to improve diagnostics and treatments, and improvement knowledge to improve processes and systems. A linkage between those two bases support improvement of outcomes.
A scientific base for improvement knowledge has been proposed, a “science of improvement” (Berwick, 2008; Bergman et al. 2015). The origin of this science could be related to the quality improvement pioneers of the early 20th century, e.g. Shewhart, Deming and Juran (Bergman & Klefsjö, 2010 Bergman 2015). The use of the term improvement knowledge (Batalden & Stoltz, 1993) relates to Deming’s elements of profound knowledge (1994) and most descriptions of a science of improvement has that stance (Bergman, 2015). Knowledge on the elements and how they interrelate is important for every improvement effort (Langley et al., 2009). The four elements of profound knowledge are elaborated on in the following.
Appreciation of a system
Entities working together to achieve the same goal could be seen as a system (Deming, 1994). The interaction between the actors in the system affects to what degree mutual goals are achieved. Knowledge on, or appreciation of, a specific actor´s role in the system in relation to other actors in the system is important in order to support the process towards the goal. What is seen as a natural way to enhance performance in one part of the system does not necessarily serve the greater goal for the whole system. By analyzing the system, in terms of organizational and individual goals and knowledge on how the system works, can support action towards greater quality. Knowledge on systems has increased since the days of Deming. Examples as Senge (1994), and Glouberman & Zimmerman (2002) have contributed to the understanding of how to understand, relate and interact with and within systems. Another contribution, a tool that takes the system into account when understanding where and how improvement projects can affect the desired outcome is the driver diagram (Langley et al., 2009). By linking the desired outcome to primary and secondary drivers, a visualization of how work with different outcomes can contribute to the overall goal is created. (See figure 8)
Understanding Variation
Variation is present in all care processes. According to Batalden and Stoltz (1993), “Understanding variation over time is a key to recognizing and using differences observed for the purpose of continual improvement”. (p 429) Variation over time, diachronic variation differs from another kind of variation present in health care settings, the synchronous variation. Synchronous variation is the variation present at the same moment. It could be the difference between patients or hospitals. Data shown on a national level, like league tables with regional comparisons (e.g. the Swedish “Öppna jämförelser”, National Board of Health and Welfare, 2015) has historically focused only on synchronous variation to show differences between regions and hospitals. The diachronic variation is powerful in assessing how a process has changed historically. A run-chart (Perla et al., 2011) is an easy way to explore variation over time by plotting data points chronologically. (See figure 1).
Distinguishing the type of variation present in a process is critical since it prompts different kinds of actions. Shewhart (1931) suggested that variation can be seen as having different causes. Deming (1986) referred to them as common causes and special causes. Common cause variation in a process could be related to a multitude of sources, but the result cannot be directly related to an event or a single cause. It is the random variation that is the product of the inherent “noise” in the system created by the variety of patients, variety of procedures and other aspects that vary over time. The result produced by the system will be predictable and the variation will stay within statistically determined limits. Along with common causes there can also be special causes, or assignable causes, an almost similar concept introduced by Shewhart (1931). Those are causes that generally are known, obvious, or can be discovered. However, when there is an assignable cause of variation, a sudden event, that affects the process, the process is not predictable within limits any longer. In a stable process with no assignable causes of variation, a fundamental change in the system is needed, to produce a better outcome. In an unstable process, that is, a process with one or many assignable causes of variation, improvement work should first focus on identifying and handling the assignable causes rather than fundamentally improve the system and its performance. Mixing up those two, the different approaches of actions determined by the types of variation, can possibly increase undesired variation. In order to use variation to track shifts and make a prognosis on future outcomes of the process, control charts can be used. Further elaboration on the use of SPC and control charts are made in paragraph 2.2.
Theory of knowledge
Gaining knowledge through the use of data in providing a rational basis for action can be done either in enumerative studies or analytic studies (Deming, 1975). Enumerative studies are made in order to draw conclusions from analysing material in a frame, often to make an estimation, to generalize from a sample. Traditional ways of generating knowledge in healthcare by studying the outcomes of treatment, like randomized controlled trials (RCTs) are in that sense enumerative. The aim is to answer the question: “Does this intervention work under ideal circumstances?” On the contrary, QI is almost always focused on analytic studies (Langley et al., 2009), studying how a process generated the material in a frame. The aim is to predict and increase possibility to choose the alternative that will be superior to the others in the future of the process under study. Improvement work is embedded in the context and this embeddedness is crucial in getting organizational learning and continuous improvement on the road (Berwick, 2008). It is important that improvement initiatives affect the whole system, so that better quality is achieved. Analytical studies focusing on time-series data are a valuable source for organizational learning and quality improvement efforts in taking action towards greater performance (Provost, 2011; Toulany, 2013). Deming proposes a view on knowledge that could be seen as pragmatic, evolving through testing. The PDSA-cycle (Plan, Do, Study and Act), or the Shewhart cycle, as Deming first put it (Moen & Norman, 2006) summarizes Deming’s theory of knowledge. Improvements and greater learning can be achieved by planning and doing experiments, studying and reflecting on the results and acting out of a broader base of knowledge acquired through the continuous cycle of experiments. (Figure 2)
Psychology
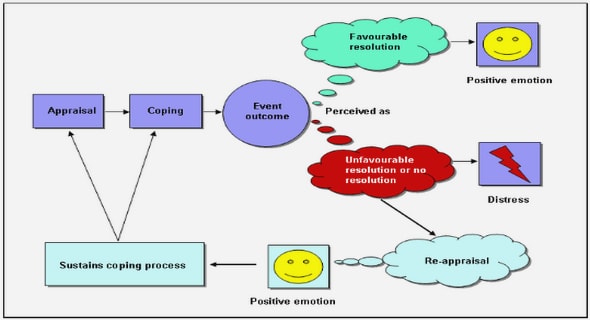
Appreciation of a system helps us understand how different parts of a system interacts in order to achieve a mutual goal while the element of psychology helps us understand the interaction between people and the context. Understanding of motivation and its central role in improvement work is crucial, since it drives behavior (Langley, 2006). Motivation is also related to values and goals. As humans we a more prone to commit to value-congruent goals and use ways of working that harmonizes with experiences and beliefs. Improvement work involves changes in how we do things or what products or machines we use. Rogers (1986) five attributes, or determinants, form a framework that can be of use in understanding the conditions related to implementing new ways of working. New ways of working in health care, just as new machines or products, can be seen as innovations. Greenhalgh (2004) defines innovations as: “a set of behaviors, routines and ways of working, along with administrative technologies and systems, which are linked to providing or supporting health care, implemented in a planned way, and discontinuous with previous practice and perceived as new by a proportion of key stakeholders, and directed at improvement.” (p. 582) The perceived usefulness and speed of diffusion of any innovation depends to a large extent on contextual factors (Rogers, 1983; Greenhalgh et al, 2004; Bate, 2014). From an adopter’s point of view, an innovation could have different attributes that possibly affect its diffusion in a certain context.
Making sense of the variation – Statistical Process Control and Control Charts
It is important to track variation over time since different kinds of variation prompts different kinds of actions. The core tools in SPC-methods are the control charts. If the data is, for example, normally distributed, random variation will stay between a upper control limit (UCL; mean + 3 sigma) and a lower control limit (LCL; mean – 3 sigma) in about 99,73% of the cases.
If all data is randomly normally distributed the process is under statistical control and “stays” within the control limits. (See figure 3) The variation in the process has “common cause variation” (Shewhart, 1931). Rules can be applied to detect when the process no longer is under control and there is a “special cause variation”; a significant event or shift in the process (Provost & Murray, 2011). Figure 4 shows one example of a signal of special cause variation. Rules on how to analyze control charts in order to track signals can be found in e.g. “The Health Care Data Guide” (Provost & Murray, 2011).
1. Introduction
2. Background
2.1 On Quality Improvement (QI) and the Science of Quality Improvement
2.2 Making sense of the variation – Statistical Process Control and Control Charts
2.3 Benefits and challenges of statistical process control and control charts
2.4 Diffusion of SPC as an innovation in psychiatry
3. Purpose
4. Methods
4.1 The Context
4.2 Method for improvement work – applying control charts
4.3 Method for the study of the improvement work – perceived usefulness
5.Results .
5.1 Results from the improvement work – applying control charts
5.2 Control Charts
5.3 Results from the study of the improvement work – perceived usefulness
6. Discussion
6.1 Revisiting purpose
6.2 Improvement work – applying control charts .
6.3 Study of improvement work – perceived usefulness
6.4 Conclusions
6.5 Implications for improvement work
6.6 Suggestions for further research
References
Appendices
GET THE COMPLETE PROJECT
Tracking Change Usefulness of Statistical Process Control in Improving Psychiatric Care