Get Complete Project Material File(s) Now! »
CHAPTER 2 REVIEW OF THE LITERATURE
INTRODUCTION
The purpose of this chapter is to present the literature relevant to the topic of study. The literature reviewed also served to explicate the findings of the study and to inform the researcher on what questions to ask during data collection. The literature review mainly focused on HIV and AIDS and on the sero-discordant couples and their experiences.
Methods of literature search
An electronic literature search was used to find information on experiences of HIV sero-discordant couples on databases such as ‘PubMed’ CINAHL, EBSCO, Proquest Central (Proquest), psychoINFO (OVID). The search was limited to publications in English. Key words included: HIV and AIDS, experiences of sero-discordant couples, Ser-discordance and discordant couples.
Inclusion criteria: The review considered any research that used the following methods: observational studies with or without interviews; systematic reviews, grounded theories; and phenomenological research to examine the experiences of sero-discordant couples. The majority of the articles that related to the following topics were included: emotional experiences of HIV sero-discordant couples, sexual experiences of HIV sero-discordant couples, psychosocial experiences of sero-discordant couples and concept papers written on sero-discordance.
OVERVIEW OF HIV AND SERO-DISCORDANCE
The HIV and AIDS scourge and the HIV discordance remain a serious medical and public health challenge. Despite the efforts made to mitigate their effects, there still remain many challenges that impact both the individual infected, persons affected, and the health needs of those affected and infected. Sero-discordance is a serious challenge in the lives of the couples especially the youth who still aspire to have children and expect to have longer and enjoyable sexual relation (Hailemarriam, Kassie & Sisay 2012:900).
Reports of sero-discordance have been reported in literature. For instance, in Uganda, Beyeza-Kasheya (2010:4) reported that up to 75% of new HIV infections take place within the HIV sero-discordant couples and about 30% of marriages are discordant. Within this group of married couples, majority of them fall within the child-bearing age and, therefore, their desire to have children is high in order to keep and own a family as well as to maintain the relationship with the spouse. HIV discordance in this situation creates a serious dilemma for fertility decision-making partners. To the infected and affected, the major challenge is with stigma, discrimination and disclosure, which by extension pose another greater challenge on HIV transmission among their partners, Naran, ( 2007:18,23 ).
The possibility that in the near future AIDS may become a chronic condition due to utilisation of antiretroviral drug and the society which is becoming aware of some coping strategies may result in some discordant couples considering a positive follow up to their desire to bear children. This decision on itself is a challenge since it calls for bravery in accepting the non HIV preventative stand in a sexual life. For both partners, the symbolic value of leading a “healthy partnership life” may be high, which might be accompanied by family pressure and societal expectation to have children. Such decision may be taken without thorough consideration of other risks, and would need consorted efforts of health care providers and a robust programme to guide the couples.
In any relationship, whether it is homosexual or heterosexual, the general expectation is that couples should live in an environment where there is serene care, understanding, support, love and sharing. Unfortunately, however, this is not always the case. Couples often times, or at least at one point in time, go through moments of stress. Cichocki (2007:2) explored the challenges faced by HIV sero-discordant couples and discovered that up to 90% of the stress causing factors among couples are the same for every relationship and the remaining 10% are the ones which are peculiar to the HIV sero-discordant couple. Cichocki (2007:3), therefore, implies that there is added stress, strain and problems within the discordant couples than in a normal relationship.
This review of literature attempts to critically explore the lived experiences of sero-discordant couples. Cichocki (2007:2) reported that 10% of all infected individuals are sero-discordant. Reviewing literature on sero-discordant assisted in the understanding of their lived experiences, their needs, and their coping strategies. It covered some of the experiences by the HIV discordant couples regionally and internationally.
Bunnel, Nassozi, Marum, Mubangizi, Malamba, Dallon, Kalule, Bahizi, Musoke and Mermin (2005:999-1012) studied the knowledge, challenges and prevention strategies of HIV discordant couples in Uganda. The study revealed that most clients lack accurate knowledge about HIV discordance. This was revealed by their expression of doubts about their diagnosis and questioning why they should engage in risk reduction measures to protect the HIV uninfected partner. There was generally a notable evidence to lack of clarity on HIV discordance which rendered them highly susceptible to popular myths and misconception such as the belief that other people are immune to HIV, and that if people engage in gentle sex they cannot contract HIV. Bunnell, Nassozi, Marum, Mubangizi, Malamba, Dallon, Kalule, Bahizi, Musoke and Mermin (2005:1002) further revealed that discordance may be marred by misconception, traditional and religious beliefs.
The bulk of the literature on sero-discordance is from East and Central Africa, and a few sources from Southern Africa and Western Countries. Literature on HIV sero-discordance is limited in Botswana and therefore very little will be discussed about Botswana. The review mainly focuses on the psychological, sexual and social experiences as well as the coping strategies for both partners involved in the HIV sero-discordant relationship.
PSYCHOLOGICAL EXPERIENCE
Bunnell et al (2005:1000) pointed out that being diagnosed with HIV causes a struggle within oneself. The diagnosis alone brings about a feeling of shock and shame. Rolland (1994:327), on the other hand describes the diagnosis of a chronic disorder as being capable of becoming a powerful third member in any daily dyadic family especially where one partner has an illness as in sero-discordant couples. Cichocki (2007:1) shares the same sentiments that there are many challenges experienced by HIV sero-discordant couples but the predominant one is stress.
Stress
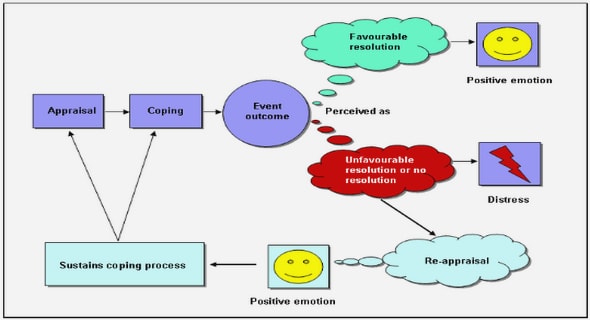
Stress is described by McCain and Huether (1998:286), as being transactional or interactional and that it stimulates our thinking processes. According to them, stress is transactionally viewed as the state of the affair arising when a person relates to situations in certain ways. McCain and Huether (1998:287) purport that people are normally not disturbed by changing or adverse situations per se, but by the way they perceive and react to them. All people have demands and when a person’s demands exceed his coping ability, there could be disturbance in cognition, emotion and behavior that may adversely affect a person’s well-being. A person with stress shows physical and psychological symptoms, such as headaches, high blood pressure, heart diseases, anxiety, depression and decreased satisfaction and interest in the environment. They also exhibit behavioral symptoms, like reduced productivity (Kay & Tasman 2006:628).
Stress in HIV discordant couples may be compounded by needs, such as money, where there is a need to consult health care practitioners. The stress was more compounded at the time when antiretroviral (ARV) medications were paid for. In some cases, the infected person may be unable to work because of ill health. If it gets to this stage, the family, mostly the infected, may experience significant stress, anxiety and resentment, especially if he/she had significant contribution to the family finances (Cichocki 2007:1). The person may also feel guilty because he/she has become the major consumer of the family resources (Cichocki 2007:1).
Stress itself can be a barrier to a successful relationship. A person who is stressed may tend to withdraw from other people who would otherwise help him/her make appropriate decisions to face the condition. At times the couple may make erroneous decision because they act impulsively out of stress and frustration.
A study conducted by the University of Medicine and Destiny of New University of New Jersey discovered that psychological distress, along with drugs and alcohol abuse are common in people who are sero-discordant (Cichocki 2007:3).
The stress in couples arises immediately after the discovery of discordance within the relationship. The uninfected partner would normally question how the other partner contracted the infection. The stress is underpinned by wondering whether the infection is the result of unprotected sex outside the relationship or a consequence of sharing needles while injecting drugs in case that the uninfected partner had no idea that they were using drugs. The stress in sero-discordant couples consists of anger, betrayal, and sadness, as the reality of their partner’s infidelity and or use of drugs set in (Cichocki 2007:3).
The same sentiments were expressed by Mabudza (2010:99) who noted that attitudes and behaviors in the sero-discordant couples are influenced by stressors and factors such as cultural beliefs, blame, guilt, anger, fear, and trust in the relationship. Fear is always a result of stigmatisation and discrimination, which ultimately causes problems of disclosure. It is also linked with constraining oneself from infecting another partner as well as how the HIV infected partner will develop AIDS.
Some studies reported that partners who are HIV discordant often times prefer to engage in sustained condom use. They therefore become overly cautious that they should not infect the negative partner (Allen et al 2003:733-740; Beyeza-Kasheya et al 2009:6). This oversensitivity may affect the couple’s liberty to participate freely in sexual activity, and as eluded to by Beyeza-Kasheyaet al (2009:6) there would be decreased sexual interest. Individuals may even stop any sexual intimacy because they fear that they would infect the HIV negative partner. In many instances this kind of action may lead to feeling of frustration, loneliness, and ultimately deteriorating relationship (Robbins 2009:2). The feeling of being a burden is also one of the major psychological issues within the sero-discordant couples.
CHAPTER 1 BACKGROUND AND ORIENTATION TO THE STUDY
1.1 INTRODUCTION
1.2 BACKGGROUND TO THE STUDY
1.3 RESEARCH PROBLEM
1. 4 PURPOSE OF THE STUDY
1.5 SIGNIFICANCE OF THE STUDY
1.6 SIGNIFICANCE OF THE STUDY
1.7 DEFINITION OF KEY TERMS
1.8 FOUNDATION OF THE STUDY
1.9 RESEARCH DESIGN AND METHODS
1.10 SCOPE OF THE STUDY
1.11 STRUCTURE OF THE THESIS
1.12 CONCLUSION
CHAPTER 2 REVIEW OF THE LITERATURE
2.1 INTRODUCTION
2.2 OVERVIEW OF HIV AND SERO-DISCORDANCE
2.3 PSYCHOLOGICAL EXPERIENCE
2.4 SEXUAL EXPERIENCES
2.5 SOCIAL EXPERIENCE
2.6 COPING STRATEGIES
2.7 THE THEORETICAL/CONCEPTUAL FRAMEWORK UNDERPINNING THE STUDY
2.8 CONCLUSION
CHAPTER 3 RESEARCH METHODOLOGY
3.1 INTRODUCTION
3.2 CONTEXT
3.3 RESEARCH DESIGN
3.4 RESEARCH METHODOLOGY
3.5 DATA COLLECTION
3.6 STUDY ETHICAL CONSIDERATIONS
3.7 DATA PROCESSING AND ANALYSIS
3.8 MEASURES TO ENSURE TRUSTWORTHINESS
3.9 CONCLUSION
CHAPTER 4 RESULTS
4.1 INTRODUCTION
4.2 BIOGRAPHICAL DATA
4.3 GETTING TO LEARN ABOUT DISCORDANCE
4.4 EXPERIENCING DISCORDANCE
4.5 EXPERIENCES OF DISCORDANT COUPLES
4.8 DISCORDANT AWARE
4.9 CHALLENGES
4.10 CONCLUSION
CHAPTER 5 STUDY DISCUSION
5.1 INTRODUCTION
5.2 SUMMARY AND INTERPRETATION OF RESEARCH FINDINGS
5.3 NEED FOR COUNSELLING
5.4 CHALLENGES IN DISCORDANT RELATIONSHIP
5.5 DISCORDANCE IN THE SOCIAL-ECOLOGICAL MODEL
5.6 CONCLUSION
CHAPTER 6 PROPOSED GUIDELINES FOR AN INTERGRATED APPROACH OF INCLUDING HIV DISCORDANCE IN THE HEALTH CARE SERVICES
6.1 INTRODUCTION TO GUIDELINES
6.2 INTEGRATED SERVICES: WHAT IT IS?
6.3 RATIONALE FOR AN INTEGRATED APPROACH IN MANAGING HIV DISCORDANT COUPLES
6.4 SCOPE AND PURPOSE
6.5 GUIDING PRINCIPLES
6.6 INTEGRATION OF SERVICES
6.7 PROPOSED MODELS FOR INTEGRATION
6.8 PROPOSED STUDY MODEL INCORPORATING MANAGEMENT OF HIV AND AIDS DISCORDANCE
6.9 BENEFITS OF THE SRH AND HIV AND AIDS-DISCORDANCE
6.10 CONSIDERING THE FAMILY/COUPLE AS A UNIT
6.11 APPLYING BEST PRACTICES IN INTEGRATION
6.12 GOVERNANCE STRUCTURE AND ROLE DELINEATION
6.13 SUSTAINABILITY
6.14 CONCLUSION
CHAPTER 7 CONCLUSION AND RECOMMENDATIONS
7.1 INTRODUCTION
7.2 RESEARCH DESIGN AND METHODOLOGY
7.3 RESULTS OF THE STUDY
7.4 RECOMMENDATION
7.5 LIMITATIONS AND STRENGTHS
7.6 THE STUDY’S UNIQUE CONTRIBUTION TO THE BODY OF KNOWLEDGE
7.7 CONCLUSION
REFERENCES.
GET THE COMPLETE PROJECT