Get Complete Project Material File(s) Now! »
CHAPTER 3 THEORETICAL FRAMEWORK
INTRODUCTION
Chapter three addresses the philosophical orientation of the thesis. The chapter describes the two models which were comparatively used to guide this study, namely, the information-motivation and behaviour (IMB) skills model and the health belief model (HBM). In addition, justification for the selection of these models is also outlined. The two models were chosen on the basis that they both emphasise on behaviour change, which is a requirement for successful PMTCT and HIV prevention and treatment in general. The similarities between the two models are further demonstrated in this chapter. It is worth noting that both models have been integrated into a PMTCT theoretical framework conducive for the Free State Province in accordance with the WHO and South African PMTCT guidelines. These guidelines are inextricably linked with other strategic policy initiatives such as the UNAIDS Global Plan towards the elimination of new HIV infections among children by 2015 aimed at keeping their mothers alive; the Strategic Plan for Maternal, Newborn, Child and Women’s Health (MNCWH); the Nutrition in South Africa 2012-2016 programme; as well as South Africa’s National Strategic Plan for HIV/AIDS, TB and STI’s 2017-2022.
THEORETICAL GROUNDING OF THE STUDY
The theoretical grounding of the study pertains to its theoretical framework. A theoretical framework refers to “the structure that can hold or support a theory of a research study. It introduces and describes the theory that explains why the research problem under study exists” (Swanson, 2013: 1). A theory provides an explanation or prediction of the relationship between concepts and constructs in a specific phenomenon in a given discipline. A theory may appear in a research study as an argument, a discussion or a figure that helps explain or predict a particular phenomenon (Creswell, 2014: 54). Theories consist of concepts and relational statements which explain, describe, predict or control phenomenon being investigated and discussed (Grove et al., 2013: 117). These philosophically founded concepts, principles and shared elements have the inherent characteristic to construct assumptions, explanations and predictions which describe why and how certain concepts are related. Theories can offer different explanations of the same phenomenon or phenomena. Furthermore, theoretical explanations and predictions are not final, but subject to change. One theory cannot be relied on as the only basis or source of absolute truth pertaining to the reality of a phenomenon or phenomena (du Plooy et al., 2014: 39-41
Conceptual framework
Polit and Beck (2017: 119) draws a distinction between the conceptual and theoretical framework, where theoretical framework is applied in the event that the study is based on a theory; whereas a conceptual framework is used when a study is based on a conceptual model. However, the above-cited authors also infer that the two terms are usually used interchangeably. The United States Department of Health and Human Services and the National Institutes of Health (2005: 4) also explain the reason for the interchangeable usage of theoretical and conceptual frameworks in health behaviour and health promotion theories, stating that: “The health behaviour and health promotion theories draw upon various disciplines, such as psychology, sociology, anthropology, consumer behaviour, and marketing. Many are not highly developed or have not been rigorously tested. Because of this, they often are called conceptual frameworks or theoretical frameworks”.
The theoretical framework outlines the theoretical scope of the study, provides guiding principles and perspective for examining the topic, helps identify key variables to be included in the study, and points the most critical research questions. The main focus of this study was on preventive health care, with some emphasis on compliance by both the health care recipients and health care providers. The relationship between non-adherence to PMTCT guidelines to HIV positivity in children aged three to eighteen months was determined by means of the mixed-methods approach to data collection and analysis. The information-motivation-behaviour skill model (IBM) and the health belief model (HBM) were adopted for this study. The two models together address the theoretical explanations of the levels of individual influence to adhere to treatment as described by the United States Department of Health and human services (2005:12), and focus on behaviour change and/or modification. In this study, these models were applied to describe the factors that influence behaviour change regarding the prevention of mother to child transmission of HIV. Firstly, behaviour is influenced by cognition. What people know and think affects how they act. Secondly, knowledge is a prerequisite for producing behavioural change, but knowledge by itself is not enough to produce most behaviour change. Lastly, perceptions, motivations, skills and social environment are key determinants of behaviour (Fisher, Amico & Herman, 2006: 463-467).
The information-motivation-behaviour (IMB) skill model
The IBM model was developed to provide an account of psychological determinants of adherence to antiretroviral treatment through the integration of various constructs from health and psychology models. It stipulates the psychological determinants of behaviour which can either improve or impair health status (Suls & Wallston, 2003: 83). Although it originally addressed adherence to ART, the model has been used to address adherence to management of other chronic diseases. In this study, it includes other PMTCT-related behaviour such as early antenatal booking, compliance to exclusive breastfeeding in the first six months, HIV testing, negotiating and maintaining consistent condom use, taking the child for HIV test at stimulated intervals, and adherence to infant PMTCT prophylaxis.
Assumptions of the information- motivation-behaviour skill model
Fisher et al. (2006: 463-467) assert that the information-motivation-behaviour skill model is characterised by the following: Individuals who are well informed, motivated and have the necessary behavioural skills are more inclined to adhere to health promotion behaviour. Secondly, individuals who are not informed, not motivated and lack certain behavioural traits are unlikely to engage in health promotion behaviour. Thirdly, personal and social motivation is also a prerequisite for the performance of health related behaviour. Fourthly, a well informed and motivated individual also needs behavioural skills to perform health promotion behaviour. Information should be understandable and applicable to the individual’s social ecology and could be in the form of health promotion messages. In the event that the information is incorrect, it could lead to wrong health promotion practices. Motivation relates to attitudes towards personal performance of health behaviour. Another construct of the model is premised on behaviour skills, which uphold that well informed and motivated individuals are able to participate in and maintain health promotion behaviour (Fisher et al., 2006: 467).
IMB’s relevance to PMTCT
Information is necessary for individuals to initiate and maintain behaviour necessary for PMTCT. According to the South African guidelines for antiretroviral therapy and PMTCT, it is mandatory that all individuals should undergo drug readiness training prior to, or during initiation of ART (South Africa, 2015b: 17). The information provided includes HIV prevention, care, and adherence to treatment. Information in the form of leaflets, posters, health education, radio and television adverts/talk shows is also provided to the population at large. Motivation is influenced by attitudes and beliefs about the susceptibility to MTCT, outcomes of the intervention and the perception of support by the significant others. Behaviour skills would be displayed by perceived ability incorporate PMTCT interventions into social life. Behaviour skill would therefore be demonstrated by early antenatal booking, adherence to ART, safer sex, administration of infant prophylaxis, exclusive breastfeeding in the first six months, infant testing at stipulated intervals, HIV testing every three months during pregnancy and breastfeeding by HIV negative mothers, as well as safer sex practices. Examples of moderating factors include maternal psychological status, socio-economic factors, risky behaviour, and HIV disclosure and partner support. The outcome of all these would be HIV negative children.
A schematic representation of the IMB skills model
Figure 3.1 below is a schematic representation of the IMB skills model and its core elements of: PMTCT/HIV Adherence Information; Moderating Factors Affecting Compliance; Behavioural Skills; Adherence Behaviour; Health Outcomes; and Motivation.
The health belief model (HBM)
The health belief model is a psychological model that tries to explain and predict people’s behaviour and attitudes towards health. It is regarded as one of the most influential models in health promotion. It was developed by Rosenstock in 1966 informed by a study on tuberculosis patients’ response to X-ray treatment. It was later extended to cover illness behaviour, preventative health, health screening and compliance to medical directives (Raingruber, 2017: 57). It now focuses on patient conformity to prescribed medical regimens and preventive and promotive health care practices.
The basic assumption of the HBM model is that individuals will take health related action in the event that they either feel that the undesirable health condition could be shunned, or have a belief that the undesirable health condition could be prevented by taking treatment and also the belief that the individual could successfully institute preventive action. According to Polit and Beck (2017: 124): “The model postulates that health seeking behaviour is influenced by a person’s perception of a threat posed by a health problem and the value associated with actions aimed at reducing the threat”. The model addresses the individual’s perception of the susceptibility and severity of the health threat and the benefit of avoiding it. It also identifies factors that affect the decision to act such as barriers, cues to action and self-efficacy. (United States Department of Health and Human Services, 2005: 13). This theory has further been developed to include six main constructs, which are: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy (United States Department of Health and Human Services, 2005: 13). Perceived susceptibility addresses the person’s belief about the possibility of acquiring the particular health condition. Perceived severity is about the seriousness of the condition and its complications. Perceived benefits address the belief that the envisaged action will prevent the adverse consequences. Cues to action are the strategies that are implemented to raise awareness, while self-efficacy is about one’s confidence in taking action. (United States Department of Health and Human Services, 2006: 13).
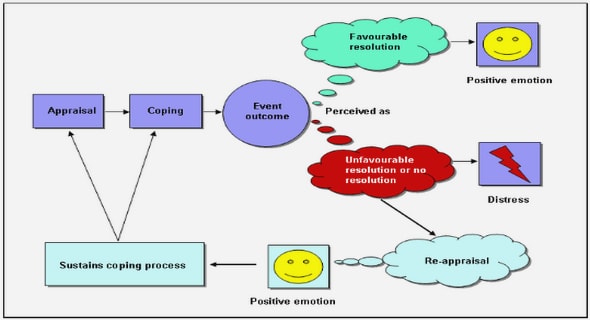
Diagrammatic representation of the health belief model (HBM)
Figure 3.2 below is a diagrammatic representation of the health belief model and its six core constructs which are centrally constituted around an individual’s perceived threat to diseases.
HBM applied to PMTCT
Figure 3.2. above is an illustration of the health belief model. All of its constructs are discussed below in relation to the PMTCT and the adherence to its prescripts as interpreted by the researcher using the model’s constructs.
Perceived susceptibility
Women or couples who believe that they are susceptible to HIV will most likely have an HIV test, book antenatal care early and institute measures to prevent the transmission to their children; whereas those who believe that they are not at risk of HIV infection will not take measures to find out if they are infected or not and will not institute measure to prevent MTCT.
Perceived severity
This construct relates to the individual’s belief about the seriousness of the medical condition and how it may affect his or her life. Individuals who believe that their conditions are serious enough to infect their babies with HIV will most likely comply with the recommended preventive measures such as exclusive breastfeeding for six months.
Perceived benefits
The main benefit of PMTCT is having HIV negative children. Therefore, mothers who believe in this outcome are most likely to adhere to PMTCT strategies.
Perceived barriers
Stigma and discrimination, non-disclosure and other psychosocial and socio economic factors may prompt the mothers not to comply with PMTCT measures.
Cues to action
Parents who are informed about PMTCT are most likely to institute action to protect their children from acquiring HIV. Information, communication and social mobilisation about HIV and PMTCT will prompt them to take preventive action, while parents who are uninformed may not be aware of PMTCT strategies.
Self efficacy
Positive attitude and confidence by parents that they can carry out measures to prevent MTCT can contribute positively to adherence.
Relationship of the HBM and IMB models
Both the health belief model and the information-motivation-behaviour skills model have been selected as the study’s conceptual and theoretical frameworks due to their affinity and relevance to PMTCT as the foundational tenet and focus of the research topic. Accordingly, Table 3.1 depicts those interstitial constructs which are similar and apply to both models in respect of Information, Motivation and Behavioural Skills.
THE CONCEPTUAL FRAMEWORK RELATED TO PMTCT
Having highlighted the seminal constructs of both the HBM and the IMB skills model, this final aspect of the chapter focuses on the implications of the two models in the PMTCT context of the study. Figure 3.2 below depicts these implications insofar as their applicability to a Free State environment is concerned.
Policy as a guide
A policy refers to “a law, regulation, procedure, administration action, incentive or voluntary practice of governments and other institutions.” (CDC, 2015). In public health, policies cover advancement and implementation of public health laws and regulations which influence individual’s behaviour towards the promotion or improvement of health (CDC, 2015). In this study, policy refers to international, national, provincial and institutional prescripts and regulations which directly or indirectly contribute to the prevention and management of HIV/AIDS, including prevention of mother to child transmission. In South Africa, there are policy guidelines which direct clinicians and all health care workers on the management of HIV among adults and children; as well as the prevention of mother to child transmission. There are related policies such as HIV testing services policy of 2016 and the infant and young child feeding policy, all of which are derived from the World Health Organisation’s and UNICEF’s guidelines. The national contraception and fertility planning policy and service delivery guidelines of 2012 also addresses the 2nd prong of the PMTCT programme and the prevention of unintended pregnancies in HIV infected women. These policies form the basis for health promotions and health education directed to all citizens to keep them informed about how to prevent mother to child transmission of HIV. There are also provincial and institutional policies which address these issues. The guideline policies also guide the clinicians and health care workers in the formulation and dissemination of information and communications messages to health care recipients during drug readiness training.
TABLE OF CONTENTS
CHAPTER 1: ORIENTATION TO THE STUDY
1.1 INTRODUCTION
1.2 THE RESEARCH PROBLEM
1.3 PURPOSE/ AIM AND OBJECTIVES OF THE STUDY
1.4 SIGNIFICANCE OF THE STUDY
1.5 DEFINITION OF KEY TERMS/ CONCEPTS
1.6 THEORETICAL GROUNDING OF THE STUDY
1.7 RESEARCH DESIGN AND METHODS
1.8 SCOPE OF THE STUDY
1.9 CONCLUSION
CHAPTER 2: LITERATURE REVIEW
2.1 INTRODUCTION
2.2 DEVELOPMENT OF THE PMTCT PROGRAMME IN SOUTH AFRICA
2.3 RISK FACTORS OF MOTHER-TO-CHILD TRANSMISSION OF HIV
2.4 INFANT FEEDING IN THE CONTEXT OF HIV
2.5 STUDIES CONDUCTED ON FACTORS THAT CONTRIBUTE TO MTCT
2.6 CONCLUSION
CHAPTER 3: CONCEPTUAL/ THEORETICAL FRAMEWORK
3.1 INTRODUCTION
3.2 THEORETICAL GROUNDING OF THE STUDY
3.3 THE CONCEPTUAL FRAMEWORK RELATED TO PMTCT
3.4 CONCLUSION
CHAPTER 4: RESEARCH DESIGN AND METHOD
4.1 INTRODUCTION
4.2 RESEARCH DESIGN
4.3 RESEARCH METHOD
4.4 DATA COLLECTION
4.6 QUALITATIVE MEASURES TO ADVANCE TRUSTWORTHINESS
4.7 QUANTITATIVE MEASURES TO ADVANCE TRUSTWORTHINESS
4.8 CONCLUSION
CHAPTER 5: DATA ANALYSIS AND INTERPRETATION
5.1 INTRODUCTION
5.2 QUANTITATIVE DATA PRESENTATION AND ANALYSIS
5.3 QUALITATIVE (INTERVIEW-BASED) DATA PRESENTATION AND ANALYSIS
5.4 Discussion of quantitative and qualitative findings
5.5 CONCLUSION
CHAPTER 6: MAIN CONCLUSIONS, RECOMMENDATIONS AND FURTHER STUDY
6.1 INTRODUCTION
6.2 CONCLUSIONS
6.3 RECOMMENDATIONS
6.3.1 Early Infant Diagnosis
6.4 POSSIBLE STUDY LIMITATIONS
6.5 CONCLUSION
LIST OF REFERENCES
GET THE COMPLETE PROJECT